


GUIDE
编者按


通信作者:杨振宇 教授
(中国人民解放军空军军医大学第二附属医院 普通外科)

作者:魏彤辉
(中国人民解放军空军军医大学第二附属医院 普通外科)
Abstract Background and Aims: Hem-o-lok clips are widely used for cystic duct and vascular closure during laparoscopic cholecystectomy (LC). Although rare, postoperative clip migration may occur, with the clip entering the common bile duct (CBD) and acting as a foreign body. Its imaging features often mimic choledocholithiasis, posing diagnostic and therapeutic challenges. Clinical awareness of this late complication remains insufficient. This study aims to summarize the clinical characteristics and management strategies through a case analysis and literature review.
Methods: The clinical data of a 29-year-old woman admitted in October 2025, four years after LC, were retrospectively reviewed. She was diagnosed with suspected CBD stones during routine examination one year prior to admission. Preoperative imaging revealed multiple filling defects in the CBD. The patient declined endoscopic retrograde cholangiopancreatography and underwent laparoscopic common bile duct exploration (LCBDE). Intraoperative findings, imaging characteristics, diagnostic process, and management were analyzed in conjunction with relevant literature.
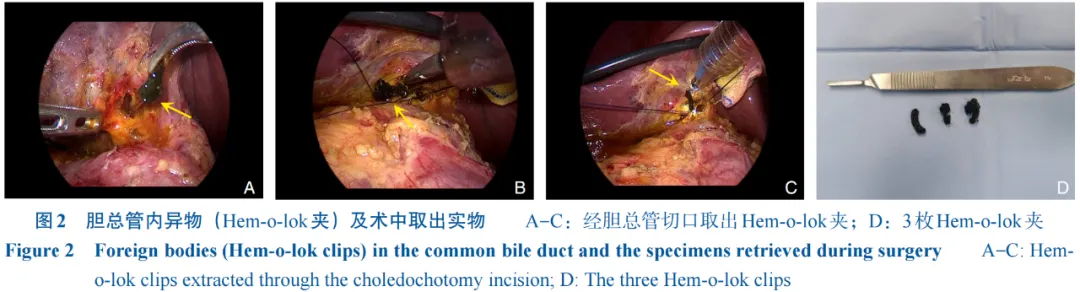
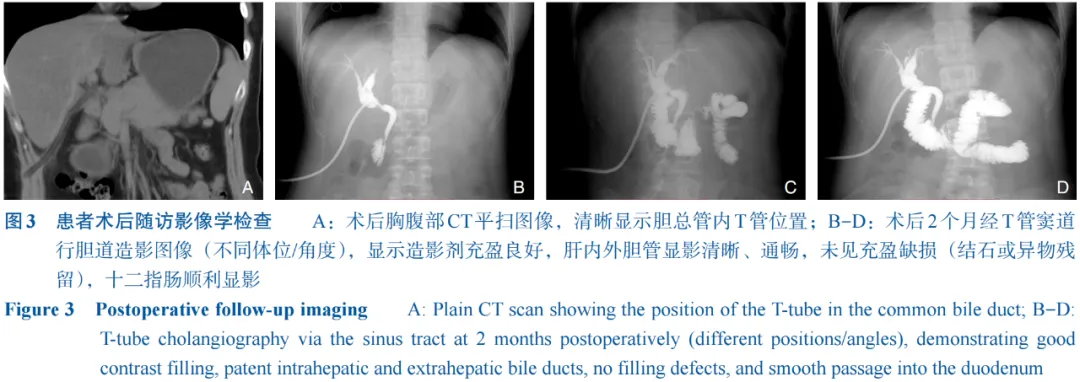
Results: Preoperative imaging suggested multiple CBD stones. During LCBDE, three migrated Hem-o-lok clips were identified and removed from the middle and lower CBD under choledochoscopic guidance. No pigment stones were observed around the clips. The final diagnosis was foreign bodies in the CBD (Hem-o-lok clips). A T-tube was placed for drainage. The patient recovered uneventfully and was discharged. Two months later, T-tube cholangiography confirmed a patent CBD without residual stones or foreign bodies, and the tube was removed successfully.
CLC number: R657.4
胆石症是一种常见的消化系统疾病,约10%~15%的成年人受其影响[1]。该病特征为胆汁成分硬化形成结石,常引发胆囊炎、胆管炎及胰腺炎等严重并发症。当前的治疗方案包括药物、内镜及外科手术等,但存在侵入性、疗程长或复发风险等局限性[2]。对于合并胆总管结石的患者,临床主要采用两种策略:腹腔镜胆囊切除术(laparoscopic cholecystectomy,LC)同期行腹腔镜胆总管探查术(laparoscopic common bile duct exploration,LCBDE),或先行内镜下逆行胰胆管造影(endoscopic retrograde cholangiopancreatography,ERCP)/内镜括约肌切开术(endoscopic sphincterotomy,EST)取石后再行LC[
1 病历资料
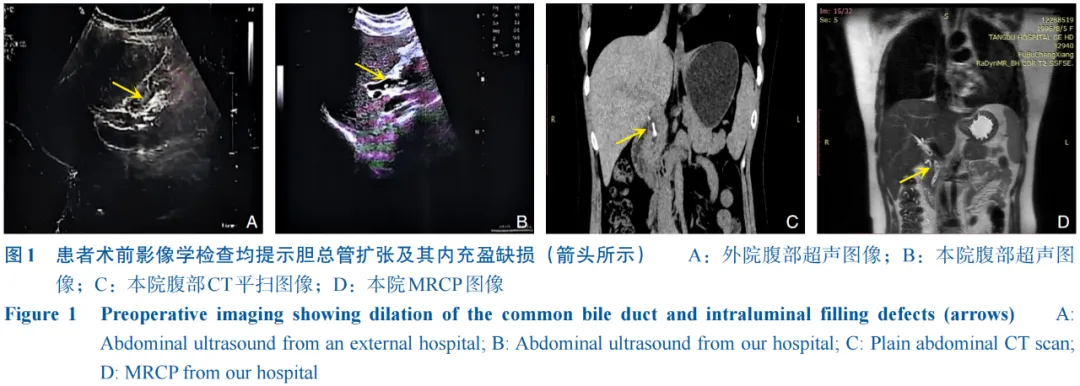
患者 女,29岁。因“体检发现胆总管结石1年余”于2025年10月12日入院。患者1年前孕检时超声首次发现胆总管结石,未予治疗,此后间断出现劳累后背部隐痛,无发热、寒战、黄疸等胆管炎典型症状。既往史值得注意的是,患者4年前因胆囊结石于外院接受LC。入院查体:生命体征平稳,腹平软,腹部可见3处长约1 cm愈合瘢痕,无压痛、反跳痛,未触及包块。实验室检查提示总胆红素23.3 μmol/L,直接胆红素9.2 μmol/L,丙氨酸氨基转移酶32 U/L,天门冬氨酸氨基转移酶23 U/L,感染指标未见明显异常。初步影像学评估:腹部超声、计算机断层扫描(CT)及磁共振胰胆管成像(MRCP)均明确提示胆囊术后缺如,值得注意的是,原胆囊三角区未见血管夹残留影。胆总管轻度扩张(直径约0.9 cm),其内见多发结节样低信号充盈缺损(图1)。初步诊断为胆总管结石、胆总管扩张、胆囊切除术后。
(在框内向上滑动手指即可浏览全部参考文献)
Branch of Biliary Surgery, Chinese Society of Surgery, Chinese Medical Association. Practice guideline for diagnosis and treatment of bile duct injury(2021 edition)[J]. Chinese Journal of Surgery, 2021, 59(6):422-429. doi:10.3760/cma.j.cn112139-20210421-00180.
[2]Batool Mirza U, Sarfaraz I, Kiran Z, et al. Melatonin's anti-inflammatory and antioxidant effects in gallstone disease: a narrative review[J]. World J Hepatol, 2025, 17(9):110964. doi:10.4254/wjh.v17.i9.110964.
[3]Sun W, Li J, Fang JB, et al. Comparison of efficacy of ERCP+LC and LC+LCBDE on cholecysto-choledocholithiasis and analysis of risk factors for recurrence of choledocholithiasis[J]. Altern Ther Health Med, 2024, 30(7):103-107.
[4]赵健楠, 刘洋, 王向, 等. 胆囊结石处理的临床决策: 从适应证到术式选择的再探索[J]. 中国普通外科杂志, 2025, 34(2):245-252. doi:10.7659/j.issn.1005-6947.250061.
Zhao JN, Liu Y, Wang X, et al. Clinical decision-making in the management of gallstones: a re-exploration from indication to surgical options[J]. China Journal of General Surgery, 2025, 34(2):245-252. doi:10.7659/j.issn.1005-6947.250061.
[5]Pavlidis ET, Pavlidis TE. Current management of concomitant cholelithiasis and common bile duct stones[J]. World J Gastrointest Surg, 2023, 15(2):169-176. doi:10.4240/wjgs.v15.i2.169.
[6]马平安, 宋春, 段春宁, 等. 腹腔镜胆囊切除术后胆总管结石复发影响因素分析及风险预测模型构建[J]. 中国普通外科杂志, 2025, 34(11):2499-2505. doi:10.7659/j.issn.1005-6947.250117.
Ma PA, Song C, Duan CN, et al. Risk factors for recurrence of common bile duct stones after laparoscopic cholecystectomy and construction of a prediction model[J]. China Journal of General Surgery, 2025, 34(11):2499-2505. doi:10.7659/j.issn.1005-6947.250117.
[7]Rogers SJ, Cello JP, Horn JK, et al. Prospective randomized trial of LC+LCBDE vs. ERCP/S+LC for common bile duct stone disease[J]. Arch Surg, 2010, 145(1):28-33. doi:10.1001/archsurg.2009.226.
[8]Shrivastava P, Nayak B, Singh P. Migrated Hem-o-Lok clips in the ureter: a rare cause of recurrent urinary tract infection[J]. BMJ Case Rep, 2017, 2017:bcr2016219143. doi:10.1136/bcr-2016-219143.
[9]Liu Y, Ji B, Wang YC, et al. Hem-o-lok clip found in common bile duct after laparoscopic cholecystectomy and common bile duct exploration: a clinical analysis of 8 cases[J]. Int J Med Sci, 2012, 9(3):225-227. doi:10.7150/ijms.4023.
[10]Huang YZ, Lin YY, Xie JP, et al. Clip-stone and T clip-sinus post laparoscopic biliary surgery: Two case reports and review of the literature[J]. World J Gastrointest Surg, 2025, 17(2):99423. doi:10.4240/wjgs.v17.i2.99423.
[11]Aminian A, Khorgami Z. Hem-O-lok clip is safe in minimally invasive general surgery: a single center experience and review of data from food and drug administration[J]. J Minim Invasive Surg Sci, 2012, 1(2):52-57. doi:10.5812/jmiss.1885.
[12]Zheng B, Li C, Wang S. A case of a common bile duct stone containing a metallic clip appearing after laparoscopic cholecystectomy[J]. Rev Esp Enferm Dig, 2023, 115(7):407-408. doi:10.17235/reed.2023.9750/2023.
[13]Zhu Z, Wang JF, Li C, et al. A case of Hem-o-lok clip migrating to common bile duct after laparoscopic cholecystectomy[J]. Asian J Surg, 2024, 47(9):4117-4118. doi:10.1016/j.asjsur.2024.05.052.
[14]Gavric A, Stefanovic S, Plut S, et al. Bile duct stone formation around migrated surgical clip 17 years after laparoscopic cholecystectomy[J]. Gastroenterol Hepatol, 2021, 44(9):662-663. doi:10.1016/j.gastrohep.2020.06.037.
[15]Dell'Abate P, Del Rio P, Soliani P, et al. Choledocholithiasis caused by migration of a surgical clip after video laparoscopic cholecystectomy[J]. J Laparoendosc Adv Surg Tech A, 2003, 13(3):203-204. doi:10.1089/109264203766207753.
[16]Ng DYL, Petrushnko W, Kelly MD. Clip as Nidus for choledocholithiasis after cholecystectomy-literature review[J]. JSLS, 2020, 24(1):e2019.00053. doi:10.4293/JSLS.2019.00053.
[17]YoshizumiT, Ikeda T, ShimizuT, et al. Clip migration causes choledocholithiasis after laparoscopic cholecystectomy[J]. Surg Endosc, 2000, 14(12):1188. doi:10.1007/s04640040030.
[18]Pradhan U, Gyawali P, Dahal R, et al. Clip migration in common bile duct: an uncommon complication of laparoscopic cholecystectomy[J]. Kathmandu Univ Med J, 2022, 20(77):111-113.
[19]Roh YJ, Kim JW, Jeon TJ, et al. Common bile duct stone development due to a Hem-o-lok clip migration: a rare complication of laparoscopic cholecystectomy[J]. BMJ Case Rep, 2019, 12(7):e230178. doi:10.1136/bcr-2019-230178.
[20]Liu DR, Wu JH, Shi JT, et al. Hem-o-lok clip migration to the common bile duct after laparoscopic common bile duct exploration: a case report[J]. World J Clin Cases, 2022, 10(19):6548-6554. doi:10.12998/wjcc.v10.i19.6548.
[21]Kou K, Liu X, Hu Y, et al. Hem-o-lok clip found in the common bile duct 3 years after laparoscopic cholecystectomy and surgical exploration[J]. J Int Med Res, 2019, 47(2):1052-1058. doi:10.1177/0300060518817216.
[22]姚驰, 王雪梅, 袁兵, 等. LC术后Hem-o-lok夹大量移位至胆总管一例[J]. 肝胆胰外科杂志, 2024, 36(11):691-694. doi:10.11952/j.issn.1007-1954.2024.11.010.
Yao C, Wang XM, Yuan B, et al. Massive migration of Hem-o-lok clips after laparoscopic cholecystectomy: a case report[J]. Journal of Hepatopancreatobiliary Surgery, 2024, 36(11):691-694. doi:10.11952/j.issn.1007-1954.2024.11.010.
[23]王一尧, 李铎, 邹瑞. LC术后Hem-o-lok夹移位至胆总管一例[J]. 肝胆胰外科杂志, 2024, 36(11):697-698. doi:10.11952/j.issn.1007-1954.2024.11.012.
Wang YY, Li D, Zou R. Hem-o-lok clip migration to common bile duct after laparoscopic cholecystectomy: a case report[J]. Journal of Hepatopancreatobiliary Surgery, 2024, 36(11):697-698. doi:10.11952/j.issn.1007-1954.2024.11.012.
[24]Álvarez Abad I, Gutierrez Grijalba O, Sarriugarte Lasarte A, et al. Migration of a clip to the common bile duct after laparoscopic cholecystectomy[J]. Cir Esp, 2017, 95(2):111. doi:10.1016/j.ciresp.2016.02.005.
[25]Rajendra A, Cohen SA, Kasmin FE, et al. Surgical clip migration and stone formation in a gallbladder remnant after laparoscopic cholecystectomy[J]. Gastrointest Endosc, 2009, 70(4):780-781. doi:10.1016/j.gie.2009.05.025.
[26]付振东, 范瑞芳, 党政, 等. 胆囊切除术后Hem-o-lok夹胆管移位3例报告[J]. 腹腔镜外科杂志, 2022, 27(12):954-956. doi:10.13499/j.cnki.fqjwkzz.2022.12.954.
Fu ZD, Fan RF, Dang Z, et al. 3 cases report of bile duct displacement with Hem-o-lok clip after cholecystectomy[J]. Journal of Laparoscopic Surgery, 2022, 27(12):954-956. doi:10.13499/j.cnki.fqjwkzz.2022.12.954.
[27]Tanimu S, Coombs RA, Tanimu Y, et al. Cholecystectomy clip-induced biliary stone: Case report and literature review[J]. J Minim Access Surg, 2025, 21(3):306-311. doi:10.4103/jmas.jmas_323_23.
[28]Vargheese S, Nelson T, Akhtarkhavari A, et al. Laparoscopic cholecystectomy in acute calculous cholecystitis: a secondary center experience[J]. Cureus, 2023, 15(6):e41114. doi:10.7759/cureus.41114.
[29]Zheng Y, Wang Y, Bai X, et al. Letter to the editor on "The cystic duct and artery were clipped using a clip applier". Nonmetal clip migration after laparoscopic cholecystectomy[J]. Asian J Surg, 2018, 41(6):585-587. doi:10.1016/j.asjsur.2018.09.001.
[30]赵海旺, 袁玉斌, 张平, 等. 腹腔镜下胆囊切除和胆总管切开取石术后Hem-o-lok夹移位[J]. 中华普通外科杂志, 2020, 35(10):819-820. doi:10.3760/cma.j.cn113855-20200402-00266.
Zhao HW, Yuan YB, Zhang P, et al. Hem-o-lok clamp displacement after laparoscopic cholecystectomy and choledocholithotomy[J]. Chinese Journal of General Surgery, 2020, 35(10):819-820. doi:10.3760/cma.j.cn113855-20200402-00266.
[31]Mills CD, McCamley C. Multiple cholecystectomy clip migration into the common bile duct causing obstructive jaundice[J]. ANZ J Surg, 2021, 91(4):E245-E246. doi:10.1111/ans.16311.
[32]Onnekink AM, Gorris M, Bekkali NL, et al. Endoscopic sphincterotomy to prevent post-ERCP pancreatitis after self-expandable metal stent placement for distal malignant biliary obstruction (SPHINX): a multicentre, randomised controlled trial[J]. Gut, 2025, 74(2):246-254. doi:10.1136/gutjnl-2024-332695.
[33]Gonçalvez GF, Barros LL, Gurgel SE, et al. Proper timing or ERCP and cholecystectomy on acute cholecystitis: a systematic review and meta-analysis[J]. Acta Cir Bras, 2025, 40:e401025. doi:10.1590/acb401025.
[34]Zhuang L, Li Y, Zhang L, et al. A comparison of the therapeutic outcomes between primary duct closure and T-tube drainage after laparoscopic common bile duct exploration: a single-centre retrospective study[J]. Wideochir Inne Tech Maloinwazyjne, 2023, 18(1):108-116. doi:10.5114/wiitm.2022.120672.
[35]汤晓东, 刘双海, 陈胜. 腹腔镜胆囊切除、胆道探查取石术后Hem-o-lok夹游走于胆总管内二例[J]. 中华消化内镜杂志, 2015, 32(8):565-566. doi:10.3760/cma.j.issn.1007-5232.2015.08.017.
Tang XD, Liu SH, Chen S. Two cases of Hem-o-lok clip wandering in common bile duct after laparoscopic cholecystectomy and bile duct exploration and lithotomy[J]. Chinese Journal of Digestive Endoscopy, 2015, 32(8):565-566. doi:10.3760/cma.j.issn.1007-5232.2015.08.017.
[36]Kandil T, El Nakeeb A, El Hefnawy E. Comparative study between clipless laparoscopic cholecystectomy by harmonic scalpel versus conventional method: a prospective randomized study[J]. J Gastrointest Surg, 2010, 14(2):323-328. doi:10.1007/s11605-009-1039-8.
[37]Bartholomew AJ, Jing C, Economopoulos KP, et al. Impact of metal vs non-absorbable, polymer clips during laparoscopic cholecystectomy[J]. Surg Endosc, 2025, 39(4):2288-2295. doi:10.1007/s00464-025-11559-x.
[38]Ravikiran HR, Niroop Sri Raghava KN, Dave P. Clipless versus clip-based cystic duct closure in laparoscopic cholecystectomy: a systematic review and meta-analysis[J]. Cureus, 2025, 17(11):e97440. doi:10.7759/cureus.97440.
[39]顾炜, 蔡兵, 吴鸣宇. Hem-o-lok夹和可吸收夹在腹腔镜胆囊切除术中的临床应用比较[J]. 肝胆胰外科杂志, 2015, 27(3):238-240. doi:10.11952/j.issn.1007-1954.2015.03.020.
Gu W, Cai B, Wu MY. Comparison of clinical application of Hem-o-lok clip and absorbable clip in laparoscopic cholecystectomy[J]. Journal of Hepatopancreatobiliary Surgery, 2015, 27(3):238-240. doi:10.11952/j.issn.1007-1954.2015.03.020.
[40]张慧林, 刘永硕, 孙象军. 胆囊术后Hem-o-lok结扎夹移位形成胆总管结石1例报告[J]. 腹腔镜外科杂志, 2022, 27(4):312-313. doi:10.13499/j.cnki.fqjwkzz.2022.04.312.
Zhang HL, Liu YS, Sun XJ. A case report of choledocholithiasis caused by the displacement of Hem-o-lok ligature clip after cholecystectomy[J]. Journal of Laparoscopic Surgery, 2022, 27(4):312-313. doi:10.13499/j.cnki.fqjwkzz.2022.04.312.
[41]顾伟刚, 陆磊, 金杭斌, 等. 腹腔镜胆囊切除术后Hem-o-lok结扎夹移位至胆道一例[J]. 浙江临床医学, 2020, 22(9):1372-1373. doi:10.3969/j.issn.1008-7664.2020.09.059.
Gu WG, Lu L, Jin HB, et al. A case of Hem-o-lok ligature clip shifting to biliary tract after laparoscopic cholecystectomy[J]. Zhejiang Clinical Medicine, 2020, 22(9):1372-1373. doi:10.3969/j.issn.1008-7664.2020.09.059.
[42]Chon HK, Jo IH, Park CH. Evolving strategies for the optimal management of common bile duct stones[J]. Gut Liver, 2025, 19(5):665-676. doi:10.5009/gnl250251.
[43]Wang X, Li Z. Management of common bile duct stones: a comprehensive review[J]. Front Surg, 2025, 12:1658784. doi:10.3389/fsurg.2025.1658784.
[44]Bessone F, Hillotte GL, Tamagnone N, et al. Ursodeoxycholic acid for the management of drug-induced liver injury: role of hepatoprotective and anti-cholestatic mechanisms[J]. J Clin Transl Hepatol, 2025, 13(2):162-168. doi:10.14218/JCTH.2024.00325.
(本文编辑 熊杨)
本文引用格式:魏彤辉, 张波, 杨振宇. 腹腔镜胆囊切除术后Hem-o-lok夹胆道移位的诊断与治疗:附1例报告并文献复习[J]. 中国普通外科杂志, 2026, 35(2):279-288. doi:10.7659/j.issn.1005-6947.250625
Cite this article as: Wei TH, Zhang B, Yang ZY. Diagnosis and treatment of Hem-o-lok clip migration into the common bile duct after laparoscopic cholecystectomy: a case report and literature review[J]. Chin J Gen Surg, 2026, 35(2):279-288. doi:10.7659/j.issn.1005-6947.250625
初审 熊 杨
复审 宋 涛
终审姜 晖
版权声明
